
The Truth About Herniated Discs
The low back pain that radiates down your leg—often described as a sharp, burning, or electric shock—is more than just an inconvenience; it can be a life-altering condition known as sciatica, frequently caused by a herniated disc. In a fast-paced city like Bangalore, where long hours spent sitting are the norm, this problem is increasingly common among the working population, from IT professionals to busy entrepreneurs.
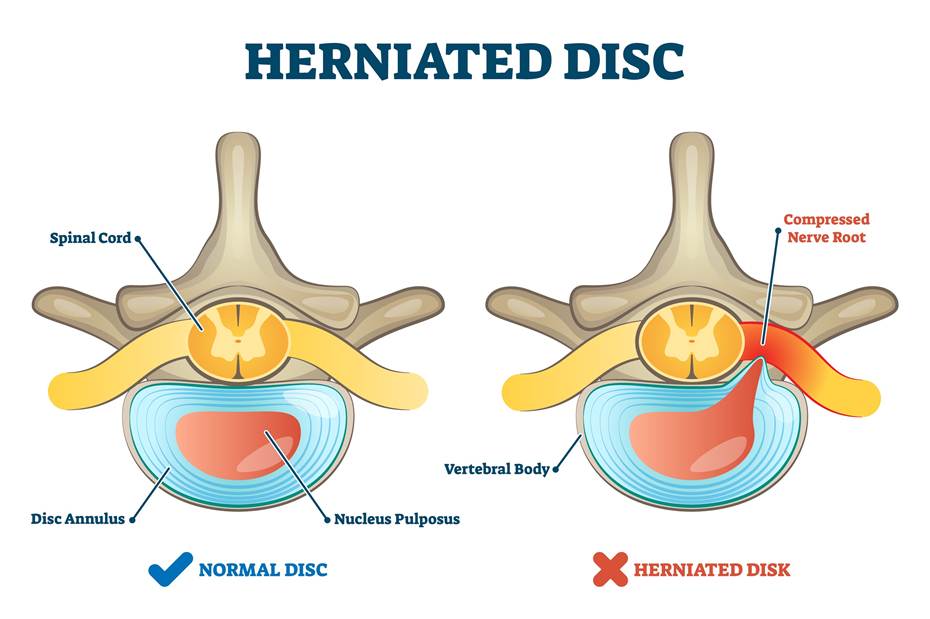
As a Consultant Spine Surgeon with years of experience treating complex spinal pathologies, I, Dr. Shashidhar B.K., understand the physical toll and psychological burden this pain carries. A herniated disc occurs when the soft, gel-like center of a spinal disc (the nucleus pulposus) pushes out through a tear in the tougher exterior (the annulus fibrosus). This extruded material can directly compress a nearby nerve root, leading to debilitating pain, numbness, and sometimes weakness.
The good news? Most herniated discs can be successfully treated without surgery. However, for a significant number of patients whose pain persists despite dedicated conservative treatment, or for those experiencing severe neurological deficits, spine surgery offers a highly effective and often immediate pathway to relief.
This comprehensive guide is designed to clarify the role of surgery in treating herniated discs, demystify the procedures, and provide you with the essential knowledge needed to make an informed decision about your spinal health journey.
Understanding the Enemy – What is a Herniated Disc?
To appreciate the treatment, one must first understand the structure involved. Your spine is a column of bony vertebrae separated by intervertebral discs. These discs are critical components, acting as both shock absorbers and flexible spacers, allowing your spine to bend and twist.
The Anatomy of the Problem
Each disc is structurally similar to a jelly doughnut: a tough, fibrous outer ring (the annulus fibrosus) encasing a soft, gelatinous center (the nucleus pulposus).
A herniated disc occurs when the nucleus pushes through a tear in the annulus. This is often confused with a “bulging disc,” where the outer ring weakens but remains intact, causing a generalized bulge. A true herniation means the central material has extruded, directly infringing on the space reserved for the spinal nerves. This pressure and the resulting chemical inflammation cause the characteristic symptoms of radiculopathy or sciatica.
Common Causes and Risk Factors
While a herniation can be triggered by a sudden trauma or a forceful lift, the primary cause is age-related degeneration. Over time, the discs lose water content, becoming less flexible and more brittle. Other significant risk factors include:
- Occupational Stress: Repetitive bending, twisting, or lifting.
- Sedentary Lifestyle: Prolonged sitting, common in Bangalore’s corporate sector, places uneven pressure on the lumbar discs.
- Obesity: Excess body weight increases the compressive load on the lumbar spine.
- Smoking: Nicotine impairs blood flow, accelerating disc degeneration.
Symptoms That Demand Immediate Attention
The most common symptom of a lumbar herniated disc is sciatica—pain radiating from the buttocks down the leg, often below the knee. Other symptoms include:
- Numbness or Tingling (Paresthesia): Along the affected nerve pathway.
- Muscle Weakness: Difficulty lifting the foot (known as foot drop) or performing specific movements.
- Cauda Equina Syndrome (Emergency): This rare but critical condition involves new-onset bladder or bowel dysfunction, numbness in the saddle area (perineum), and severe weakness. This necessitates emergency surgical intervention.
The Non-Surgical Road – When is Surgery NOT Needed?
It is crucial to emphasize that spine surgery is almost always a last resort for chronic pain. The vast majority of patients—approximately 90%—will find significant relief and recovery through conservative management alone. The goal is to allow the body time for the inflammation to subside and the disc fragment to potentially shrink or be reabsorbed.
The Cornerstones of Conservative Treatment
- Rest and Activity Modification: Temporary avoidance of activities that aggravate the pain (lifting, prolonged sitting).
- Pharmacological Management: This may include Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), muscle relaxants, and specific nerve pain medications (like Gabapentin or Pregabalin).
- Physical Therapy (PT): A structured PT program focuses on restoring mobility, strengthening the core muscles (the natural corset of the spine), improving posture, and teaching proper body mechanics. PT is indispensable, whether surgery is performed or not.
- Spinal Injections: Epidural Steroid Injections (ESIs) are a highly effective tool. Administered directly into the epidural space near the compressed nerve root, they deliver potent anti-inflammatory medication (corticosteroid) to reduce swelling and pain, buying the patient time to benefit from physical therapy.
Determining the Surgical Timeline
Surgery only becomes a practical and appropriate discussion when the patient’s severe, debilitating pain persists for 6 to 12 weeks despite a dedicated course of aggressive conservative therapy, or if there are signs of progressive neurological damage. We rely heavily on objective evidence from an MRI to confirm the mechanical compression of the nerve before considering surgery.
The Surgical Decision – When is Spine Surgery Indicated?
The decision to proceed with spine surgery is never taken lightly. It is a shared discussion between the patient and the spine surgeon, guided by objective criteria.
Absolute and Relative Criteria for Intervention
| Criterion | Definition | Urgency |
| Intractable Pain | Pain that is severe, chronic, and unresponsive to 6-12 weeks of non-operative care. | Relative |
| Progressive Neurological Deficit | Worsening muscle weakness, increasing numbness, or loss of reflex confirmed on clinical exam. | Relative/Urgent |
| Foot Drop | Inability to lift the front part of the foot due to nerve damage. | Urgent |
| Cauda Equina Syndrome | New-onset bladder/bowel dysfunction and numbness in the saddle area. | Absolute Emergency |
The central goal of surgical intervention for a herniated disc is decompression—to safely remove the disc fragment that is pressing on the nerve root and restore the nerve’s health. It is a precise, targeted intervention designed to relieve nerve compression and alleviate sciatica immediately.
The Gold Standard Procedure – Microdiscectomy
For the vast majority of herniated discs in the lumbar spine, the gold standard treatment is a Microdiscectomy (MD). This procedure has been perfected over decades and, when performed by an experienced surgeon, offers one of the highest success rates in all of orthopedic surgery.
What is a Microdiscectomy?
A microdiscectomy is a minimally invasive surgical procedure used to remove the portion of the herniated disc material that is irritating the spinal nerve. The key to its precision and success lies in the use of high-power magnification.
The Minimally Invasive Spine Surgery (MIS) Approach
In modern spine centers like the Bangalore Spine Specialist Clinic, the microdiscectomy is performed using Minimally Invasive Surgery (MIS) techniques:
- Small Incision: A tiny incision, typically only $1$ to $2$ centimeters, is made over the affected area.
- Magnification: The surgeon utilizes a high-powered operating microscope or specialized loupes. This allows for brilliant illumination and magnification of the delicate spinal nerves and disc material, ensuring only the necessary fragments are removed.
- Muscle Sparing: Unlike traditional open surgery, which required stripping muscles away from the spine, MIS techniques use small tubular retractors to gently push the muscle aside. This minimal muscle disruption is the central reason for faster recovery, less post-operative pain, and reduced scarring.
The Procedure Step-by-Step
The MD procedure is precise and focused:
- A small incision is made in the lower back, verified using fluoroscopy (real-time X-ray).
- Specialized retractors are used to create a small working corridor to the spine.
- A small window of bone (laminotomy) may be created to access the spinal canal.
- The nerve root is carefully identified and gently moved aside.
- The herniated disc fragment is identified and meticulously removed using specialized micro-instruments.
- Crucially, only the extruded fragment is removed, preserving the remaining healthy disc tissue to maintain spinal stability.
- The instruments are removed, and the small incision is closed with a few stitches.
Outcomes and Success Rate
Microdiscectomy boasts an exceptional success rate, typically over 90%, for relieving the primary symptom of leg pain (sciatica). Patients often feel an immediate, sometimes dramatic, reduction in the radiating pain upon waking from surgery. It is important to manage expectations: while leg pain relief is excellent, relief from chronic low back pain (which often involves other degenerative changes) can be more variable. We manage expectations realistically before surgery.
Cervical Discectomy Considerations
While microdiscectomy is the primary choice for the lower back (lumbar spine), disc herniations in the neck (cervical spine) are often treated differently, as the spinal cord itself is present at this level. The two most common procedures are:
- Anterior Cervical Discectomy and Fusion (ACDF): Removing the disc through the front of the neck and fusing the adjacent vertebrae to stabilize the segment.
- Cervical Disc Replacement: Replacing the damaged disc with an artificial mobile disc, preserving motion at that segment—an excellent option for younger, active patients.
Advanced Surgical Techniques and Alternatives
While the microdiscectomy is the workhorse for most herniations, I utilize other advanced techniques when the pathology requires a different approach, always prioritizing the least invasive option that provides a definitive solution.
Endoscopic Spine Surgery
This is the next generation of minimally invasive spine surgery. Instead of an operating microscope, a small tube and camera (endoscope) are used. The key advantage is an even smaller incision (often less than 1 cm), allowing for the procedure to sometimes be performed under local anesthesia. Endoscopic techniques are often utilized for specific types of contained herniations or lateral recess stenosis, offering superior visualization of the lateral nerve roots.
Lumbar Laminectomy/Decompression
If the herniated disc is accompanied by significant spinal stenosis (a narrowing of the spinal canal) due to thickening ligaments or bone spurs, simply removing the disc fragment may not be enough. A laminectomy involves removing a portion of the lamina (the bony roof of the vertebra) to create more space for the nerve roots and spinal cord. This is often combined with a discectomy to address both the herniation and the overall crowding.
Spinal Fusion (When Instability is Present)
In certain complex cases, such as a large recurrent herniation, the presence of instability (vertebra slippage, or spondylolisthesis), or severe chronic back pain alongside nerve compression, the surgeon may need to stabilize the segment after decompression. Procedures like TLIF (Transforaminal Lumbar Interbody Fusion) or PLIF (Posterior Lumbar Interbody Fusion) involve removing the entire disc and replacing it with a bone graft or cage, fusing the vertebrae together to eliminate painful motion and stabilize the spine. This is a much larger surgery and is reserved only for specific, necessary indications to preserve long-term spinal function.
Recovery and Life After Surgery
The rapid recovery associated with minimally invasive techniques is one of their greatest benefits, distinguishing modern spine care from procedures of decades past.
The Immediate Post-Operative Period
- Hospital Stay: Most patients undergoing a microdiscectomy are walking within a few hours of surgery and are discharged within 24 hours. Fusion procedures typically require 2-3 days.
- Pain Management: Post-operative pain is typically well-managed with oral medication, and is usually a muscle-soreness pain, vastly different from the agonizing nerve pain the patient experienced pre-operatively.
Rehabilitation and Return to Activity
Rehabilitation is essential to a long-term, successful outcome and requires patient commitment.
- First 1-2 Weeks: Focus on walking, avoiding the “BLT” motions (Bending, Lifting, Twisting). Office workers can often return to a desk job within this window.
- Physical Therapy (PT): Starts shortly after surgery. The focus is initially on body awareness and gentle movement, progressing to rigorous core stabilization exercises. PT helps rebuild muscle strength and, crucially, minimizes the risk of disc re-herniation.
- Full Recovery: Most patients can return to light activity and driving within 2-4 weeks. Unrestricted activity or sports are typically approved after 8 to 12 weeks, pending the surgeon’s final evaluation and the patient’s recovery milestones.
Minimizing Recurrence
While the success rate is high, there is a small risk (around 5-10%) of the disc re-herniating. This risk is managed effectively by: maintaining a healthy weight, quitting smoking, and—most importantly—adhering strictly to the physical therapist’s guidelines for lifelong core strengthening and proper lifting mechanics. The surgery removes the protruding fragment, but only lifestyle changes protect the remaining disc.
Conclusion: Taking the Next Step in Bangalore
A herniated disc diagnosis is daunting, but the path to relief is clear. While conservative treatments are always the first approach, modern, minimally invasive spine surgery, particularly the microdiscectomy, offers a reliable and highly effective solution for those whose lives are limited by chronic sciatica.
At the Bangalore Spine Specialist Clinic, we prioritize an individualized, patient-centered approach. We use state-of-the-art diagnostic tools and advanced surgical techniques to ensure the best possible outcome. If chronic sciatica is limiting your life, don’t wait. Schedule a consultation with Dr. Shashidhar B.K., Consultant Spine Surgeon, to get an accurate diagnosis and discuss a tailored treatment plan designed to get you back to a pain-free life.
Call us today to understand how we can help you find lasting relief and reclaim your quality of life.